
Pain is invisible. That means any time, any place, someone can just kick you in the stomach by telling you that your pain is ‘all in your head’.
That’s why it is so important for the people we love to believe us when we describe what we feel and it’s why we so value medical professionals who listen and take us at our word.
Nonetheless, the truth is, pain IS in your head. So is everything else you see, hear, or perceive. So is what we know.
Our brain is the part of the nervous system that interprets and integrates multiple inputs (and creates some of its own). Knowing that allows us to use our knowledge of how the brain interprets and integrates information to reduce the experience of pain both immediately and over the long term.
The first part of this series talked about the implications of the International Association for the Study of Pain’s revised definition of pain. This post focuses on the second part.
Pain is . . .

(Please look back at the six caveats and extensions the society lists in their definition – they’re important.)
Both sensory and emotional experiences can cause pain. The definition implies that the emotional pain that we feel resembles or is associated with the sensations we feel when we experience actual or potential tissue damage. In other words – pain is pain.
Linking external with internal & thoughts with emotions
Both physical pain and emotional pain activate the anterior insula and the anterior cingulate cortex. Both of these areas process the emotional components of physical pain and the emotional components of pain caused by social rejection (for example, being rejected by someone we love).
The anterior insula processes the connection of the outside world and our emotions, as when we see horrific, revolting, or disgusting things. It is the source of that visceral connection you feel in your gut at an upsetting smell, taste, or sight. It’s why we physically shudder in horror and feel nauseated when we’re grossed out.
The anterior cingulate cortex connects the limbic system (which regulates emotions) with the prefontal cortex (which in involved in thought and judgement). Its primary function is control and processing of negative emotions.
In sum, both physical and emotional pain activate and are processed by areas of the brain that:
- Link emotion/activation and thought/cognition
- Link external stimuli and emotional reactions
- Focus on experiencing, processing, and controlling negative emotions.
Whether we feel “hurt” or rejected or are physically injured, these same areas are activated. Pain triggers an emotional response. Emotional responses can trigger pain.
The Bio-Psycho-Social Model of Pain
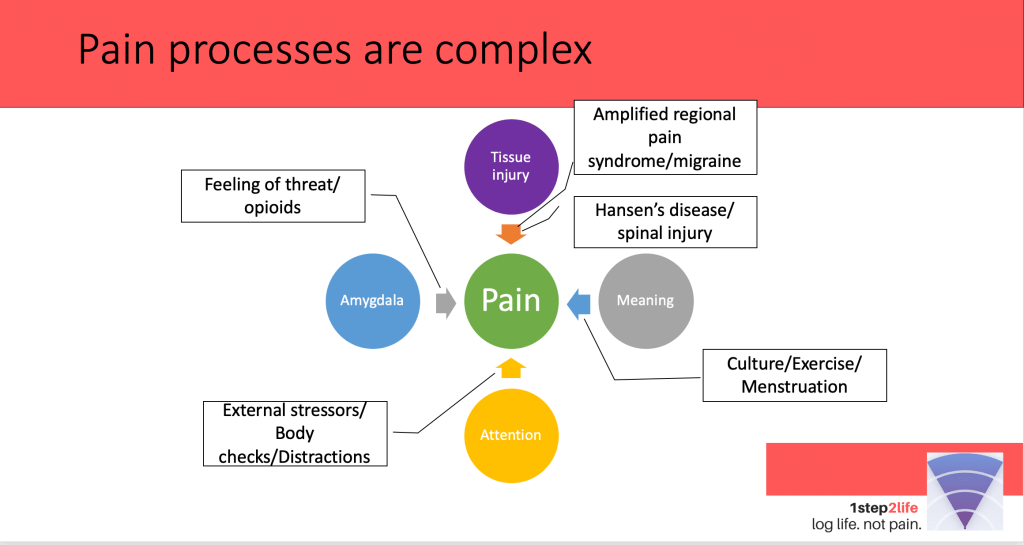
The bio-psycho-social model of pain makes this connection between external stimulus and internal processing explicit.
Experienced pain is a function of
- Real or threatened tissue damage with resultant nervous system activation
- Perceived threat and activation (shown by the amygdala, here)
- The cultural interpretation and meaning we give to the stimuli
- How much of our attention is focused on the stimuli
It’s easy to find clear examples of how people’s experience of pain can be increased or decreased at each of these points.
Tissue injury & nerves. Nerve damage that interferes with healthy pain processes makes people with diabetic neuropathy vulnerable to injury because they can’t feel damage occuring. For example, my aunt could not feel (and therefore didn’t properly care for) a blister in her foot that became infected and eventually resulted in an amputation. In this case, tissue injury occurs but isn’t passed on to the brain for appropriate protective steps. Pain did not do its job.
At the other hand, the nerves of people with Amplified Regional Pain syndrome send information to the brain signaling extreme tissue damage. The body responds accordingly and the person is often in extreme pain. However, there is no tissue damage. The injury is to the nervous system sending a faulty signal.
The amygdala, anterior insula, and anterior cingulate cortext. The way we interpret stimuli – the meaning we give it – is partially dependent on the amygdala, anterior insula and anterior cingulate cortex. When we feel safe or we understand the source of stimuli to be non-threatening, we don’t interpret it as pain. When we’re stressed, nervous, or scared, we do.
Think for example, of the physical sensations of a hard workout. You’re out of breath. Your heart is racing. Your legs are aching. – maybe even shaking You’re in a sweat. You feel exhausted. At the gym you might think of this as a good sign – you’re getting strong! You might feel exhilarated by these sensations. Waking up from a sound sleep with these identical sensations would be terrifying. Context and emotional state matter.
The importance of mental state is one reason that so many pain rehabilitation programs emphasize yoga, meditation, and other stress reduction practices as ways to reduce pain. When we are calm and don’t feel threatened, pain is easier to deal with.
Meaning. One of the clearest empirical examples of how meaning changes our perception of pain is menstruation. Girls who have been brought up to believe the menstruation is scary or taboo report much more pain during their periods than those who don’t. The physical sensation is the same for both groups, but pain perception differs.
Interestingly, the way opioids work is not by interfering with the physical stimuli of pain. Instead, opioids take away the emotional component of pain so it is observed but not responded to as threatening.
Attention. Pain demands our attention, but pain also diminishes when we take our attention away. It’s kind of like itching. If you start thinking about itching, you will start to itch all over. You may be feeling fine right now, but if I asked you where you hurt, a quick body check would probably reveal many small points of irritation.
On the flip side, you may be in a great deal of pain right now. However, if you were focused on something very engaging (a funny comedy routine, doing mental math, an important conversation, playing a video game), the pain would recede somewhat from your consciousness. One reason the 1step2life app asks how often you want to log your pain is that many people find logging their pain and paying attention to it makes pain worse. That’s why we let you decide.
Harnessing the model’s power
One of the strengths of the bio-psycho-social model is that it offers multiple avenues to attack chronic pain.
Medical professors typically focus on that first step: interfering with the disease process. When pain goes on to become persistent, however, the other parts of the model become more important in the experience of pain. This includes sensitization of the nervous system to pain and greater likelihood that neutral (or even positive) stimuli will be perceived as pain. In chronic pain, pain is the disease, not a symptom.
Emotional and cognitive interpretation – understanding – of pain and sensation, the meaning given to pain and how threatening we see it, and how much we focus on it all influence how we experience pain and how easy or hard it is to cope with it.
Lifestyle changes like stress reduction, pain education, and increased engagement – particularly in enjoyable, meaningful, and distracting activities – help people living with pain by utilizing the power of the model.
Research suggests that making these changes improves happiness and coping and reduces depression in the short term. But long term, they decrease pain. It seems as if just as our nervous system can train itself to feel pain all the time, it can also be retrained to stop.
That is the reasoning behind 1step2life.
Check out the 1step2life app!
Start where you are. Set your own goals. Take back your life. A tool for tracking goals, emotions, and success, not just logging pain. And the only app that has a mode specifically for parents, partners, and other carers that supports effective coaching and strong relationships.

Comments
2 responses to “Pain Is In Your Head. It’s Still Real.”
[…] It can be part of a multi-disciplinary approach to treating chronic pain. Here, I talk about the bio-psycho-social model of pain, focusing on different parts of the pain process and how they can be […]
[…] of heat/pain information in the brain is complicated and varies between people because it is tempered by memory and emotion. That being said, the trigeminal nerve is processing everything from a fly landing on your cheek to […]