
Physics has gravity (it’s not just a good idea, it’s the law).
Psychology has learning theory. The basic ideas behind learning theory are deceptively simple:
- If you are rewarded for something you will do it more often.
- If you are punished for something, you will do do it less often.
- If something bad is happening and it stops, you’ll do whatever it is that stopped it again.
- If something good is happening and it stops, you’ll be less likely to do that in the future.
It’s one of the hard things about treating chronic pain. Often, getting up and out increases your pain short term. making you more likely to withdraw or stay in bed, and less likely to get up and out in the future. From a technical perspective, your actions were punished.
Similarly, if you do something to try to stop pain – biofeedback, for example – and nothing happens, you’re less likely to do it again. You got no reward for your effort.
Learning theory is so well established, psychologists rarely study it any more. We just use it. I use it when I train my dog. It’s basic to parenting and management classes. It’s foundational to special education.
Learning theory is easy to define, but difficult and tricky to apply. (A true story illustrating this point is here.) It is also quite subtle. For example, it varies with age, with teens being relatively more sensitive to short term rewards and less sensitive to punishment than older people are. (This is an important part of the design of 1step2life, as I explain in this video.)
I’ll be writing more about basic learning theory and it’s application later in this series.
Social Learning Theory and Efficacy
Right now I’d like to talk about SOCIAL learning theory.
B.F. Skinner’s work on reward and punishment taught us a lot about both animal and human behavior.
Albert Bandura’s social learning theory gave us even more insight into why we don’t always behave in the way that Skinner would have predicted. Introducing cognitition (thinking) to the basic ideas of reward and punishment is a critical component of learning theory – and marks the change from learning theory to social learning theory.
We learn from watching others. One of the important lessons of social learning theory is that we learn from watching others being rewarded and punished. If I see someone trying a treatment and it helps, I’m much more likely to try it myself. I learn from their reward vicariously. If I know something hasn’t helped a friend, I am less likely to try it myself.
I am most likely to learn from others like myself. I am also more likely to learn from others who I see as like myself. For example, girls are more likely to emulate the behaviors than their mothers than fathers. If a treatment is suggested that worked for someone I know who has a similar condition and I see as a lot like myself, I’ll probably give it a go if it worked for them. The less like me the person I have knowledge of is, the less likely I am to learn from their experience.
Three components of action
I don’t do everything I know how to do.
There are lots of behaviors that we know HOW to do but don’t enact. I know how to smoke a cigarette. Three of my grandparents were two pack a day smokers – I’ve watched them smokethousands of time. But I’ve never smoked. Why?
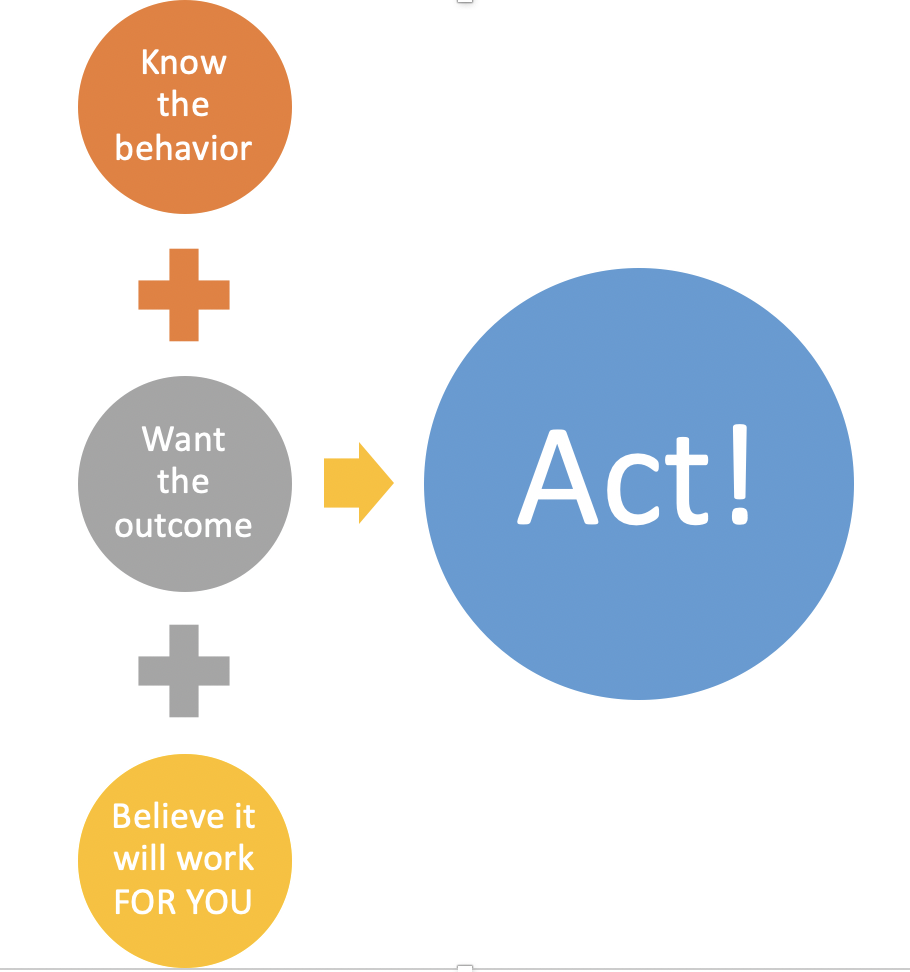
This is where the social efficacy part of Bandura’s social learning theory comes in. He argues that several things have to happen for us to enact a behavior.
- Want the outcome. First, you need to want an outcome. Let’s take biofeedback as an example. Research suggests that biofeedback and other forms of stress reduction can make it easier to cope with pain and can reduce pain over time. That desired goal increases the likelihood that you’ll try biofeedback.
- Know the behavior. Second, you need to know the behavior. If no one teaches you how to do it, you won’t use it.
That’s pretty basic. You’re not going to do it if you don’t WANT what it gets you or if you don’t KNOW HOW to do it.
The third component is more complex.
- You need to believe it will work FOR YOU.
Let’s unpack that.
First, you need to believe that biofeedback is an effective stress reduction technique. Plus, you need to believe that stress reduction is helpful in reducing pain IN GENERAL.
If you don’t think stress reduces pain OR if yu don’t think that biofeedback reduces stress, you aren’t going to use biofeedback even if you’ve been taught how to use it.
This is one reason that educating ourselves is so important.
Reading about how the amygdala changes the experience of the pain, for example, might increase your belief that stress influences pain, even if that connection isn’t immediately obvious. Knowing that, in turn, might increase your belief that stress reduction might be helpful to you. Further reading on biofeedback or studies of its efficacy might also increase your belief that biofeedback is an effective technique. Knowing people who have used it and found it helpful could also help.
Bottom line: You need to believe something will help in order to do it. If you don’t think it will work, you won’t
FINALLY, you need to believe that biofeedback will work FOR YOU. This is important. My son is really really good at using biofeedback effectively. For years, it was the ONLY thing that reduced his pain. However, if you believe that you’re not the kind of person who meditates, or that biofeedback works for some kinds of pain, but not for yours, or if you think it’s something that some people can do, but you just have no talent for, you’re not going to try.
Why? Because although you believe it may work for others, you don’t think it will work for you.
That’s what efficacy means. Believing something will work. Self-efficacy, means believing it will work for you.
Why do something that’s hard if you don’t think it will help you?
Efficacy and self-efficacy are key components of all behaviors.
Chronic pain, depression, anxiety, and other long-term conditions rarely just go away with time. They take treatment and effort.
Most of those treatments require the active participation of the person suffering. Even if that act is making a call to the doctor. Or picking up a treatment at the pharmacy. And certainly if it is something like physical therapy, going to work or school in pain, or the discipline of biofeedback.
Stuck? Diagnosing the problem
If you’re having trouble starting and keeping going, look to see where the problem might be.
If there’s something you want and you’re not acting to get it, maybe it’s time to ask yourself why.
- Do you really want the goal? You’ve thought about exercising more or going to school or getting out of bed earlier. It’s not happening.
It’s not happening.
Ask yourself: Is this really a goal you want? And, if so, do you want it more than the effort you think it will take to get it? (In other words, what’s your cost-benefit analysis?)- If yes keep reading. Identify your sticking point.
- If you want it, but think it’s too ‘expensive’ evaluate. Is there any way to make it easier to reach all – or part – of your goal? In other words, can you make the reward worth the cost?
- If no, don’t worry about it. Focus on the goals that are more achievable or will make you happier.
- Do you have the skills? A lot of times goals like reducing pain are complex and we don’t know where to start. Or they can feel overwhelming because there are so many things you can do that you don’t know where to start.
- Start somewhere. If there is one thing you think will help and you know how to do, start there.
- If you don’t know how, learn. Want to try biofeedback and don’t know how? Try YouTube. (We’re also starting a new series on it next week.) Don’t know how to get one of the new migraine drugs? Call your doctor. Join a support group. Ask for help. None of us can do this alone.
- Do you believe it will work? Physical therapists have a problem. People are injured. PTs prescribe an exercise regime. It hurts (punishment) and it’s boring (more punishment). PTs know from lots of research, that doing the exercises will help. The problem is that almost NO ONE does the exercises.
Why? Clients don’t believe it will help. It just seems stupid. It’s too simple. And it’s hard. And it’s boring. So they don’t do it.
Same thing with lots of the components of pain rehabilitation.
If you know there’s something you should be doing and you know how to do it and it’s not getting done, ask yourself: Do I really believe it will work? And, if so, do you really believe it will work FOR YOU?
If not, you’re probably not going to do it. So you’re going to have to ask yourself. Why? And what next?
I will be talking next week about growth mindsets, efficacy, and how differnt people deal with setbacks.
Because all of this is hard. And it takes action that we can only do ourselves.
Check out the 1step2life app!
Start where you are. Set your own goals. Take back your life. A tool for tracking goals, emotions, and success, not just logging pain. And the only app that has a mode specifically for parents, partners, and other carers that supports effective coaching and strong relationships.
